
What is Ulnar Neuropathy?
Ulnar neuropathy is the second most common nerve compression problem (after carpal tunnel syndrome). It is more common in men than woman likely due to some differences in anatomy between genders.
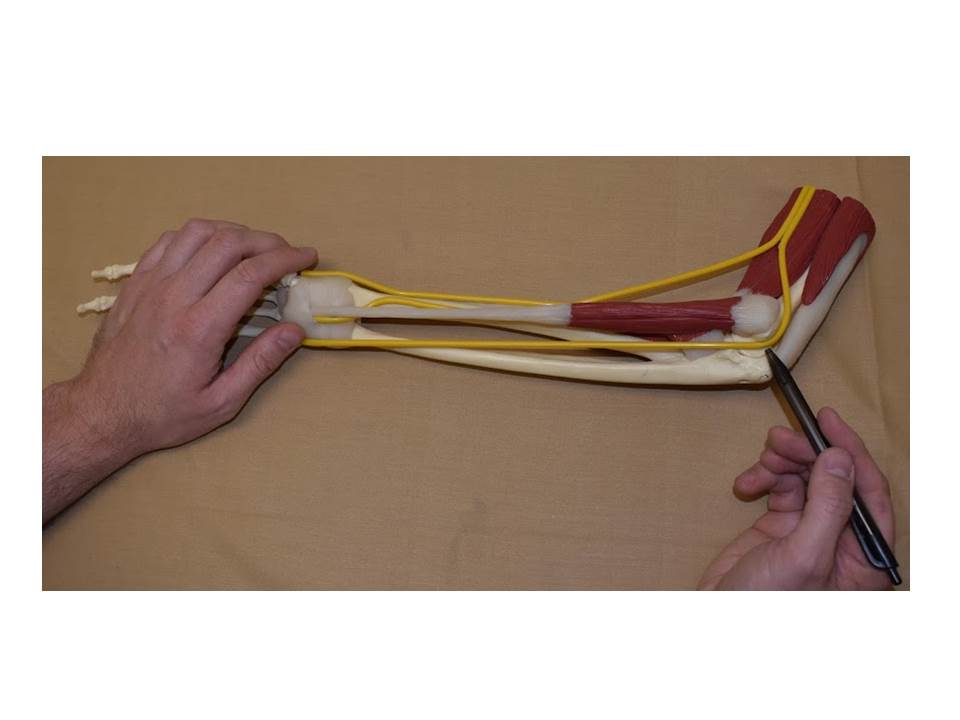
Ulnar neuropathy is not a disease. It is a mechanical problem where the ulnar nerve at the elbow becomes compressed (pinched). The ulnar nerve travels down the inner part of the arm and wraps around the inner elbow before passing into the forearm and hand. The ulnar nerve travels through the “cubital tunnel” at the elbow with (Osborne’s) ligament over top. There is also a muscle connective sheet (aponeurosis) overtop the nerve. This nerve is the “funny bone” nerve; the one that when you bang your elbow shoots sensations down to the hand. You may be able to feel parts of the nerve if you straighten your arm out and rub the groove on the inside edge of your elbow.
Neuropathy simply refers to an injured nerve. When the ulnar nerve becomes irritated from injury or from pressure it can lead to ulnar neuropathy.
What does the ulnar nerve do?
The ulnar nerve receives sensation information for the ring, pinky finger, and that side of the palm/hand. This nerve also controls many of the small muscles of the hand. These include muscles that spread the fingers apart, cross your fingers, and some that help move the thumb. The muscle that bends the pinky finger is also connected to this nerve.


What are the symptoms of ulnar nerve dysfunction?
When a nerve isn’t working properly you might experience numbness or tingling in the hand due to compression of the sensation nerves. When damage is more severe it causes weakness of the muscles which reduces grip strength and reduces control for fine movements like writing, typing, texting, and doing up buttons.
How is ulnar neuropathy diagnosed?
Ulnar neuropathy is diagnosed by a combination of history, physical examination, and nerve function testing (nerve conduction studies).
Patients suffering from ulnar neuropathy most commonly complain of numbness and tingling in the ring, little finger, and palm on that side of the hand. Some people experience it radiating up to the elbow. The tingling is often worsened when there is direct pressure on the inside of the elbow or when the elbow is kept in a bent (flexed) position such as talking on the phone or sleeping.
In some patients pain may also be present at the inside of the elbow where the nerve is located. Nerve damage can progress to the point of muscle weakness in the hand, which can result in these muscles getting smaller (atrophy).
For the most part ulnar neuropathy is a numbness/tingling problem. Pain at the inside of the elbow experienced with physical activity is most commonly due to tendon and bone (tendonitis/arthritis) problems. If there is also numbness and tingling down into the ring/pinky finger then ulnar neuropathy is a possibility. Some people also experience cramps in some of these hand muscles as part of the ulnar neuropathy.
The physical examination by the doctor includes testing your arm and hand strength, reflexes, and sensation. The doctor is looking for patterns of lost nerve function including reduced sensation and hand weakness. Often in mild to medium cases the physical examination is normal.

Nerve conduction study (NCS) is an objective test that measures the function of the nerve. When the nerve is compressed it slows down the nerve signals at the elbow. The NCS detects the slowing of the signals. When more severe damage occurs the size of the nerve responses are reduced.
How did I get ulnar neuropathy?
Part of the problem is how the elbow works. The ulnar nerve actually stretches when the elbow is bent (flexed). Keeping your elbow flexed for prolonged periods can contribute to ulnar nerve damage. The most common offender is sleep. Usually when we are sleeping, we sleep with our elbows flexed (not straight). Other habit postures during the day like holding your head up with your hand or typing with elbows flexed more than 90 degrees can contribute. Talking or using electronic devices (with the elbow flexed) has been such a common cause; it has been termed “cell-bow”.
Direct pressure to the inside of the elbow over time can also be very damaging to the nerve. The nerve can become irritated from innocent things like leaning on the elbow while you sit at a desk, using a computer, resting elbow while driving, or while running machinery. Other job duties where you lean on your elbow might also contribute.
In some instances ulnar neuropathy can be caused by changes to the anatomy at the elbow. Bony build up (osteophytes) from arthritis at the elbow can contribute to compression of the nerve. People who have previously had elbow fractures, dislocations, or arthritis might not be able to fully extend their elbow anymore. This leads to a kind of constant stretch of the nerve.

What treatment options are available for ulnar neuropathy?
Ulnar neuropathy is a condition that you have the most control of in preventing progression or even improving. The key things to remember throughout your day are:
- Avoid pressure at the inside of the elbow where the nerve is vulnerable.
- Keep the elbows semi-extended (greater than 90 degrees) as much as possible throughout the day
If possible, try to limit the amount of time you do tasks which require a lot of elbow bending. This is called activity modification. The nerve tolerates brief periods of stretch but sustained stretch can cause injury. If possible try to keep the elbow extended more than 90 degrees at all times.
Limit activities to keep pressure off the inside of the elbow, such as, leaning on armrest, table tops while on computer, or car doors while driving.
If possible sleep with your elbow semi-extended to avoid stretching the nerve. It doesn’t have to be rigid straight. Light sleepers who toss and turn can keep positioning their elbows semi-extended. Back sleepers who sleep with their hands resting on their chest should change their habits. Some people find that sleeping with a pillow under your arm (sort of hugging it), is enough to keep the elbow extended more than 90 degrees.

If symptoms don’t go away by modifying your habits or the nerve damage is more serious your doctor may advise you to wear a prescribed elbow brace to sleep with. These braces can be purchased off the shelf (pre-fabricated) or occasionally custom made. Their function is to keep the elbow straight while you are sleeping. It’s easy to go to sleep telling yourself you will keep your elbow straight, but after the lights go out it is often out of our hands!

(Picture courtesy of Diamond Athletic Medical Supplies)

(Picture courtesy of Diamond Athletic Medical Supplies)
Surgery is the required treatment if things don’t improve with activity modification and bracing.
When should I go back to my doctor?
There are two components to the experience of function loss from ulnar neuropathy. The first symptoms are intermittent tingling in the hand; usually with elbow flexed or leaning on the elbow. At first this may only be with sustained periods of pressure or flexion. As it progresses, the hand will go numb with short or minimal periods of pressure/stretch. It is best to catch it at this stage.
If the hand is frequently going numb or feels like it is almost constantly numb despite activity modification and elbow bracing, you should contact your doctor to consider reassessing the nerve function by repeat nerve conduction study or being referred for surgery. A sense of weakness in the hand is also a reason to be reassessed or have surgery.
What happens if I don’t seek treatment and the ulnar neuropathy progresses?
The next stage is permanent numbness where the tingling/numbness are there constantly to some degree. While it may feel odd or uncomfortable, lack of sensation in the pinky finger doesn’t usually affect hand function very much. The next stage in progression is loss of motor function with weakness and muscle shrinkage (atrophy). Weakness due to ulnar neuropathy affects the hand ability to perform fine motor activities (e.g. using nail clippers), as well as grip strength. In general it is the weakness that impacts someone’s function more severely.
When numbness has become constant or atrophy has set in; the ulnar neuropathy has become severe. When cases become severe in this way, it might not fully respond to surgery. The number one goal of ulnar neuropathy surgery is to prevent progression. Even after a technically successful surgery, patients might be left with some permanent numbness and hand weakness in these severe cases.
What can you tell me about ulnar neuropathy surgery?
There are two general types of ulnar neuropathy surgery: decompression and transposition.
A simple ulnar nerve decompression surgery is usually the preferred surgery; at least to begin. This surgery involves division (cutting) the hard fibrous ligament (Osborne’s ligament) and muscle connective sheet (aponeurosis) overtop the nerve. This relieves the pressure from the nerve. This is the surgery that most patients will have. For some people the decompression by itself doesn’t work and they have to go on to have the transposition surgery.
Ulnar nerve transposition surgery is more technically complicated, slightly more risky, but protects the ulnar nerve better longterm. The compression of the nerve by the ligament is one of the problem. The other problem is the stretch as the elbow is flexed. Transposition surgery involves freeing up the nerve along the inner arm and sliding it in front of elbow. After a successful transposition the nerve can be felt in front of the elbow instead in the path/groove in between the bones. Once moved, the nerve is slack and can no longer be stretched or pinched by leaning at the elbow. While transposition surgery is felt to be better at fully protecting the nerve, this surgery involves more extensive cutting of tissues. Often this results in increased swelling and pain with a longer recovery. A transposition surgery is usually the preferred surgery if there is significant bony buildup from arthritis in the joint or if the elbow can’t be fully extended.
Ulnar nerve surgery is a day surgery meaning you are in and out the same day. Often it requires being put under with a general anesthetic. Your surgeon will talk to you about your anesthetic options.
Like anything in medicine there are potential risks. Post-operative pain and infection are most common. Occasionally people can experience persistent elbow pain after surgery. Rarely the nerve can be damaged further through the surgery. I have only seen this a handful of times in more than 10 years. This risk is greater with the transposition surgery.
Recommendations for time off work: This varies by the surgeon, technique, and what kind of work you are returning to. Usually return to heavy work/lifting is expected between 6 – 8 weeks. Less physically demanding activity like typing, or writing can happen much sooner.
Recovery of nerve function after surgery depends on how severe the nerve was damaged and how long it had been affected. Mild-medium cases where patients are experiencing intermittent hand tingling is expected to go away quickly after surgery. In more severe cases where there is some constant numbness in the fingers or shrinking (atrophy) of the hand muscles the recovery can be prolonged. Depending on the severity of injury, nerve recovery will be greatest by 12-18 months.
In severe cases, the broken nerve fibers have to regrow from the elbow into the hand and fingers. This is a very slow process that can take up to 12-18 months. Despite a successful surgery and time for the nerve to heal, some people will be left with permanent numbness and weakness in the hand if the nerve damage was too severe and prolonged. The most important success of ulnar neuropathy surgery is to prevent nerve damage from getting worse.
Ulnar neuropathy surgery is generally not a surgery to relieve pain: It is important to note that some people (though not most) can have pain at the inside of the elbow with ulnar neuropathy. Ulnar neuropathy is mostly a numbness/tingling problem. If the biggest symptom is elbow pain, and numbness/tingling is minor then tendonitis/arthritis diagnoses should be considered. Ulnar nerve surgery for the main goal of improving elbow pain is often not successful.
