
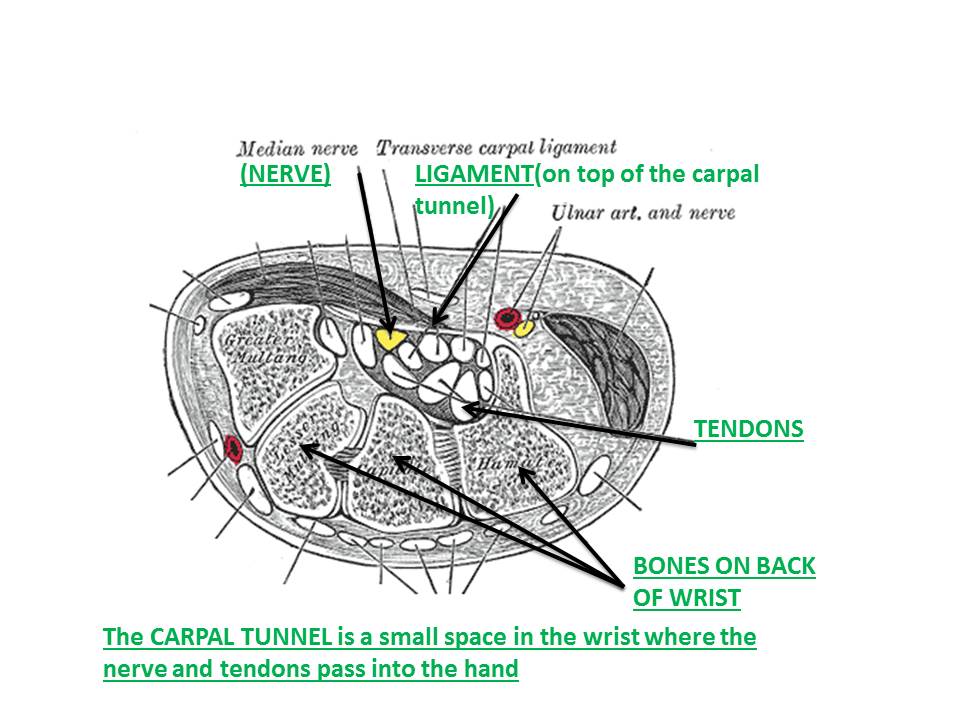
What is Carpal Tunnel Syndrome (CTS)?
Carpal Tunnel Syndrome is not a disease, it is a mechanical condition where the median nerve in the wrist becomes compressed (pinched). The median nerve travels with tendons through the “carpal tunnel” made up of wrist bones and a ligament over top. Carpal tunnel syndrome commonly affects both hands but might be worse in one more than the other.
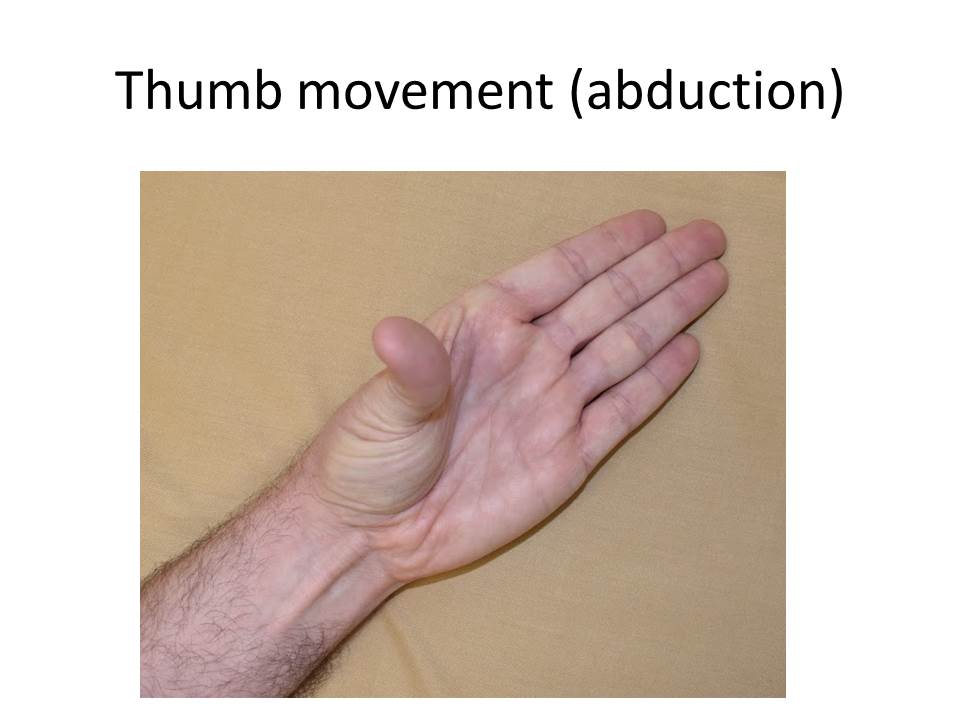
What does the median nerve do? What are the symptoms of nerve dysfunction?
The median nerve receives sensation information for the palm side of the thumb, index, middle, and half of the ring finger. This nerve also controls the muscle that moves the thumb. Holding you hand palm up, try pointing your thumb to the ceiling. This is the muscle controlled by the median nerve. When a nerve isn’t working properly you might experience numbness or tingling in the hand due to compression of the sensation nerves. When damage is more severe it causes weakness of the muscle that moves the thumb.

How is it diagnosed?
Carpal tunnel syndrome is diagnosed by a combination of history, physical examination, and nerve function testing (nerve conduction studies).
The typical symptoms in carpal tunnel syndrome are numbess and tingling in the thumb, index, and middle finger. Most people say that it just feels like the whole hand is going numb. Sometimes only a couple of fingers are affected (e.g. middle and ring finger). This tingling usually wakes people up in the middle of the night, or is more severe when they first wake up in the morning. Activities that require sustained grip or arm elevation may bring on these symptoms during the day. Common triggers are driving a car, reading a book, or holding a phone where the hand goes numb and you must drop the hand down for the feelings to go away.
For the most part carpal tunnel syndrome is a numbness/tingling problem; it is NOT a pain problem. Some people experience pain in the wrist and forearm in the middle of the night (with the numbness). Some people get pain in the thumb muscle in the palm during the day. Generally speaking; pain in the hand and arm during the day while doing things is NOT due to carpal tunnel syndrome. Daytime pain is usually due to other problems like arthritis or tendinitis. It is common that patients with carpal tunnel syndrome will have other musculoskeletal conditions that cause pain in their hands and arms.
The physical examination by the doctor includes testing your arm and hand strength, reflexes, and sensation. The doctor is looking for patterns of lost nerve function including reduced sensation and thumb weakness. Often in mild to medium cases the physical examination is normal.
Nerve conduction study(NCS) is a sensitive and objective test that measures the function of the nerve. When the nerve is compressed it slows down the nerve signals. The NCS detects the slowing of the signals. When more severe damage occurs the size of the nerve responses are reduced.
How did I get CTS?
Carpal tunnel syndrome is very common. It is more common in women than men and more common as we get older though it can occur at any age. Some people are predisposed to it by genetics where there will be a history of close family members having carpal tunnel surgeries in their 30’s or 40’s. The ligament that covers the carpal tunnel like a sheet of plastic gets harder as we get older which is one reason why it is associated with age.
Sometimes carpal tunnel syndrome is “provoked”. Conditions that cause swelling in the wrist area can contribute to nerve compression. CTS is common during pregnancy due to swelling in hands and legs. Inflammation in joints/tendons in rheumatoid arthritis, or swelling from untreated hypothyroidism can also cause nerve compression. After surgery or an injury to an arm, swelling can pool in the hand and cause CTS. Nerves that are less healthy in general (such as in people with diabetes) are less resistant to physical stresses and are predisposed to develop carpal tunnel syndrome.
Physical activities can contribute to CTS. Activities requiring repetitive wrist flexion/extension, forceful grip, and vibrating tools are risk factors for developing CTS. Work and hobbies can lead to CTS in this way. Often patients are able to trace back to a change in the amount or kind of activities they are doing with their hands at work, exercise, or hobbies. The relationship between occupational typing and CTS is not clear.
What treatment options are available for CTS?
Your doctor will almost always prescribe wrist braces because it is a cheap, safe, and easy treatment. Wrist braces are worn at night to keep the wrists straight. When we sleep, we often flex our wrists. That flexion pinches the nerve and is part of the reason why people wake up at night with the tingling feeling. Keeping the wrist straight gives the nerve a chance to heal. Wearing braces 24 hours a day or only at nighttime was studied; they are equally effective. For that reason we recommend that patients only wear braces to sleep. Some patients find the brace seems to make things worse, If this happens try loosening the brace. In many braces there is a plastic stick that makes it uncomfortable. If it is hard to tolerate try taking it out.


In some instances, carpal tunnel syndrome is provoked by a change in your physical activities. By avoiding those triggering activities involving repetitive movements, forceful gripping, and use of vibrating tools you may be able to help the nerve heal. This activity modification may include your work duties, exercise habits, or hobbies.
Corticosteroid injections (“cortisone shots”) have proven benefit in the treatment of carpal tunnel syndrome. They are often offered if there is a sudden onset severe case or if someone is looking for relief of symptoms while waiting for surgery at a later date. These injections are performed in the clinic at the bedside. The needle is placed in the carpal tunnel beside the nerve. Relief from the injection tends to last between 3 and 6 months. Injections can be repeated. In very severe cases the injections may have reduced benefit.
There can be some soreness in the wrist but it is generally not a very painful injection. Possible complications includes a skin infection, skin depigmentation (white spot) at the injection site, or allergic reaction to medicine. In theory an injection into the nerve could cause further damage but that has not occurred in the more than 10 year history of the clinic.
There are many other treatments that have been tried but none that have convincing scientific evidence of benefit. Nerve gliding (or nerve flossing) is a technique where exercises are using to increase the mobility of the nerve in hopes of reducing symptoms. Studies have shown that these techniques are possibly beneficial. (Carpal Tunnel Exercises)
Carpal tunnel surgery is the cure if symptoms persist despite braces and injections. It is a very good surgery with more than 90% success rate.
When should I go back to my doctor?
Bracing alone is quite successful in treating mild carpal tunnel syndrome. Mild-medium cases often benefit from both bracing and possible steroid injections. If symptoms persist despite bracing (and possibly injections) you should return to your doctor and ask for a referral for surgery. In many people CTS symptoms occur mostly at night. Even if bracing settles the night time symptoms, worsening of daytime symptoms should be recognized as a sign of progression. If symptoms begin to happen frequently during the day or occur with minimal activity (e.g. holding a spoon) then you should consider surgery.
In cases where symptoms have been going on for a long time (more than a year), braces might help temporarily but surgery will often be required. If NCS results determine medium or severe changes your doctor may recommend going straight to surgery to prevent further nerve damage and possibly permanent loss of function.
What happens if I don’t seek treatment and the carpal tunnel syndrome progresses?
Carpal tunnel syndrome progresses from the numbness/tingling being at night, to during the day intermittently, to eventually being constant. When numbness is constant it means it has become severe. When sensation in the hand is lost it causes loss of coordination and often dropping objects. Very severe carpal tunnel syndrome causes atrophy (shrinking) of the thumb muscle. When cases become severe in this way, it might not fully respond to surgery. Even after a technically successful surgery, patients might be left with some permanent numbness and thumb weakness in these severe cases .
What can you tell me about carpal tunnel surgery?
Carpal tunnel surgery is a very common and technically straight forward surgery. The goal of the surgery is to divide (cut) the transverse carpal ligament that is putting pressure on the nerve. That’s it. It’s a highly successful surgery with more than 90% effectiveness. Rarely patients may have recurrent carpal tunnel syndrome requiring a second surgery but that doesn’t happen often.
It is a day surgery meaning you are in and out the same day and typically takes less than an hour. Often there would just be local anesthetic to freeze the skin rather than being put under with a general anesthetic.
There are 2 techniques: open vs. endoscopic. Open surgery means an incision is made at the base of the palm so the surgeon can directly get at the ligament. Endoscopic surgery is a “keyhole” surgery where a small incision is made in the forearm and a scope device is used to divide the tendon from inside the wrist. The endoscopic surgery involves less cutting of tissues, which usually means less swelling and pain with a quicker recovery. The endoscopic surgery is more technically challenging and performed by fewer surgeons. This usually means greater wait times.
Like anything in medicine there are potential risks. Infection, and post-operative pain are most common. Occasionally people can experience persistent wrist pain after surgery called “pillar pain”. In more than 10 years I have only seen a handful of times where a patient’s nerve was worse or damaged through surgery. The transverse carpal ligament (cut during surgery) acts like a pulley. After surgery some patients report a minor reduction in their grip strength.
Recommendations for time off work: This varies by the surgeon, technique, and what kind of work you are returning to. Usually return to heavy work/lifting is expected between 4 – 6 weeks. Less physically demanding activity like typing, or writing can happen much sooner. Quickest return to work is with the endoscopic surgery.
Recovery of nerve function after surgery depends on how severe the nerve was damaged and how long it had been going on for. Mild-medium cases where patients are experiencing intermittent hand tingling is expected to go away quickly after surgery. In more severe cases where there is some constant numbness in the fingers or shrinking (atrophy) of the thumb muscle the recovery can be prolonged. The intermittent nature of painful tingling at night should still go away soon after surgery. In severe cases the broken nerve fibers have to regrow from the wrist into the fingers. This can take up to 9-12 months. Despite a successful surgery and time for the nerve to heal some people will be left with permanent numbness and weakness in the hand if the nerve damage was too severe and prolonged.
